In Britain, the National Health Service (NHS) is not so much admired as revered. It is more than just a state-funded, free-at-the-point-of-access health service: it is a profoundly politicized cultural icon, imbued with nostalgia for the postwar social contract and the “golden age” of the welfare state.1 Even when its day-to-day function is the target of frustrated criticism, the program that the NHS embodies—free health care delivered to all, irrespective of need—is emotively praised and fiercely defended by politicians across the spectrum. In 2020, then UK Prime Minister Boris Johnson called the NHS a “national asset” and “the beating heart of this country.” “It is unconquerable,” he said, and “powered by love.”2 The emotional politics of the NHS are felt when even relatively parochial decisions about health service resourcing, planning, and policy become vexed and controversial. The N for “national” in the NHS means that local decisions can be drawn into wider, often fractious debates, ones that tie the pragmatics of hospital building to arguments about what it now means to be British.
This is the charged ideological context that makes the idiosyncratic history of one hospital building, Guy’s Tower, particularly informative. Guy’s Tower is an unusual building whose political and architectural development are intertwined. Its history is correspondingly rich and tangled, and can be read as a microcosm of modern British history.


Guy’s Hospital dates from 1721, when it was founded in London by the philanthropist Thomas Guy as an institution for “incurables” discharged from the nearby St Thomas. Guy’s bequest, made possible in part by buying low and selling high during the South Sea bubble, was one of the largest charitable endowments to be made in eighteenth-century London. The magnitude of the gift ironically resulted in a decline in philanthropy in London for the rest of the century, and spirited posthumous attacks on Thomas Guy’s character.3 In order to support the reputation of the founder, Joseph Nickolls was commissioned to paint a large ceiling oval, The Apotheosis of Thomas Guy, showing Guy robed as a Protestant clergyman, rather than dressed as a merchant, ascending to heaven. After Guy’s death, the hospital grew richer through canny investments and the profits of vast properties in Herefordshire. By the twentieth century, Guy’s Hospital had accumulated unusual wealth and influence.
German bombs dropped on the south bank of the Thames during the Second World War destroyed much of the original monumental building, including The Apotheosis of Thomas Guy, although the hospital itself continued to function throughout the war. For thirty years the site remained partly derelict. In 1974, the hospital chose this historical site to build a thirty-four-story tower, nestled against another monument to mid-century hospital design: New Guy’s House, the country’s first postwar surgical block, completed in 1961. Both buildings were part of a redevelopment plan designed to centralize all clinical services in the hospital, leaving the older, eighteenth and nineteenth-century buildings for staff living quarters and teaching space for medical and nursing students. The tower was designed by architects Watkins Gray and not only provided a new home for the dental school and hospital wards, but also housed a new boiler room for the whole complex, providing infrastructure that by 1974 was very much overdue.
The Hospital Plan
In 1948 the new Labour government established the NHS, nationalizing a patchwork of health services that had hitherto been run by local authorities and was heavily dependent on what John Mohan calls the “vigour of voluntarism.”4 Hospital infrastructure itself was in a dire state: 45% of institutions had been built before 1891.5 Across the country, the Ministry of Health (MoH) found a “pattern of deficiencies, outmoded physical facilities, maldistribution and uneven quality of services … owing to either poverty or neglect.”6
Despite the sweeping administrative reorganization and increased demand that came with the foundation of the NHS, as well as the poor quality of existing infrastructure, the pace of hospital construction immediately after 1948 was remarkably slow. In 1962, the Daily Mail reflected on British hospital architecture: “The average large city hospital is a grim, grimy, forbidding relic of the Victorian age, out of date and out of place.”7 Histories of the British welfare state have shown that this sluggish progress was a product of politics and policies at both a central and local level. Austerity imposed by the Treasury along with Aneurin Bevan’s resignation as Minister of Health in 1951 meant that what money there was, was funneled towards housing and education (£430m and £57m respectively), rather than healthcare (just £10m). As Jonathan Hughes puts it, “The most remarkable feature of the new NHS hospital service’s capital allocation during the 1950s was its insignificance.”8
By 1953, anxieties about NHS spending prompted the MoH to appoint a Committee of Enquiry into the Cost of the NHS, known as the Guillebaud Committee. The committee’s 1956 report showed that the NHS was actually financially healthier than had been feared, and so spending stringency was eased. In the early 1960s, the MoH conducted a review of existing hospital services. In 1962 Enoch Powell, then Conservative Minister of Health, published the Hospital Plan for England and Wales. As Alistair Fair has shown, the Hospital Plan was just one of several contemporary “modernizing plans,” including the Robbins Report on higher education (1963), the Buchanan Report on traffic planning (1963), and the Parker Morris Report on the design of housing (1961).9 Like the other plans of the early 1960s, the Hospital Plan was inspired by a commitment to planning as a way to fundamentally re-order society and welfare state.10
The Hospital Plan aimed to produce a network of district general hospitals with 600–800 beds that served populations of around 100,000–150,000.11 In January 1962, the Daily Mail celebrated that England’s Victorian-era workhouses were to be “replaced by something as modern as, say, the latest office block.”12 The plan itself was similarly optimistic:
The Hospital Plan will determine for many years to come the broad lines of development of the hospital service, and indeed of the Health Service as a whole. No other nation has had—or taken—the opportunity to refashion its hospitals so comprehensively and on so large a scale.13
The realization of the plan’s proposals, however, was incomplete. While hospital planning was not the only aspect of the welfare state that attended to the nation as a whole, it unusually advanced a “centralized approach” to “provision and design.”14 By contrast, the design of schools, housing, and universities remained the prerogative of local authorities. In order to overcome the essentially devolved nature of the NHS, enacting the plan would necessitate pragmatic collaboration with the regional bodies responsible for hospitals.15 While health expenditure rose in the 1960s, wider initial optimism about the possibility of reimagining the built environment, and the idea that planning could be directed towards the making of new kinds of medicine and, indeed, citizenship, soon faded.16 Costs spiraled, and the plan was eventually superseded in 1974 by administrative reorganization.
The Hospital Plan has been the subject of much recent scholarship, and this narrative of hope to disappointment is a familiar one.17 But some exceptional hospitals, like Guy’s, succeeded in realizing their architectural visions. The tower makes clear the influence of an overlooked aspect of hospital rebuilding and design: charity. While all NHS hospitals were state-funded, many teaching hospitals had been allowed to retain their substantial endowments, and Guy’s used that financial heft not just to pay for part of the project, but to expedite its progress, supersede the interests of the MoH, and influence the tower’s form, use, and design.

Hospital Charity
Prior to the NHS, there was a mixed economy of healthcare in Britain. Voluntary hospitals, funded by charitable donations, shared space with private institutions, general practitioners, and the old Poor Law workhouses. When the health service was nationalized, some of the wealthier English teaching hospitals, like Guy’s, were reluctant to surrender their funds to state control. As with so many aspects of the early NHS, a compromise between healthcare professionals, individual institutions, and the government had to be struck. English teaching hospitals could keep their endowments, provided they only spent their money on things that weren’t critical to the delivery of NHS services. They could use their endowments to fund research or pay for “staff and patient amenities”—added extras like Christmas parties, mess rooms, and ward window boxes. They could receive donations, but could not fundraise, and they could not spend their money on more fundamental things like clinical equipment, staff salaries, or buildings and capital projects.
For those unfamiliar with the NHS, its histories, cultures, and conventions, it might seem strange that its founders were so hostile to charity and, particularly, the use of endowments in the building of healthcare institutions. Surely the benevolence of individual donations could work hand in hand with the collective benevolence of the welfare state? However, prior to the foundation of the NHS, healthcare in Britain relied on the uneven distribution of charitable and philanthropic support. People living in wealthier and more populated areas, therefore, had access to better quality healthcare. More money was also directed to subjects of sympathy—like cancer patients, orphans, and the “deserving” poor—rather than being equally dispersed to all citizens.
The principles of the early NHS were antithetical to this uneven distribution. The service’s visionary, Minister of Health Aneurin Bevan, was driven by the belief that access to services should be based on clinical need, not an individual’s ability to pay, and also not based on where a patient lived, what kind of life they led, or what kind sickness they suffered from. It was therefore baked into the NHS’s founding principles that charity would have only a very circumscribed role in the provision and funding of healthcare. In theory, these principles lasted until around 1980, when Margaret Thatcher’s Conservative government made it possible for hospitals to run fundraising campaigns again, and to spend their money more liberally to supplement exchequer contributions.
The welfare state, then, from its inception in 1948 until 1980 was committed to the idea that a nationalized health service ought to be funded by public taxation and accountable to the state. However, both policy and practice were far more complex than this relatively straightforward account might make it seem. While the MoH initially insisted that endowments could not be spent on building projects, by the mid-1950s, they had already watered down their earlier objections. For example, in their 1955 report, the Hospital Endowment Commission wrote, “We thought it right that Boards should not be precluded from applying endowments for building purposes.”18 Indeed, the original 1946 NHS Act noted that teaching hospitals could use their endowments “for such purposes relating to hospital services.”19 The language here was vague enough to allow a considerable amount of discretion on behalf of individual hospital boards when it came to spending their charitable donations.
Guy’s Hospital, 1948–1974
Guy’s Hospital was and remains one of the wealthiest hospitals in the UK. But in this period, for the most part, it played by the rules. The endowments committee was chaired by Iris Brook, an ex-nurse and avowed socialist. The committee’s minutes are full of instances when she refused to spend charity money on NHS services, concerned that doing so would undermine the principles of the welfare state and reduce the amount of exchequer monies available to the hospital. Her concerns were at once ideological and practical. She aligned herself with the ethics of the early NHS with respect to the place of charity and was also reluctant to do anything that might jeopardize Guy’s future financial health. If the hospital were to make it clear that it did not need to rely on state funds because of its ample endowments, then the state might withdraw future funding. But nobody is perfect and, in the 1960s, Guy’s spent a vast sum of money—money that was not supposed to be spent on capital projects—in order to circumvent MoH interference, expedite the building of the new hospital tower, and shape its form, design, and function according to the institution’s specific needs.
Guy’s rebuilding plans had been in play since at least 1947, as a result of the considerable bomb damage caused during the war. On June 5, 1963, hospital representatives met with officers from the MoH to discuss their proposed tower block scheme. At the meeting, the ministry accepted that the hospital needed to expand, and agreed in principle that the tower block comprised “the next stage in the Hospital’s development.”20 Emboldened by this tentative approval, the hospital immediately set up their own Tower Block Building Committee. This motley assemblage of medical, dental, and nursing staff, as well as medical and lay administrators, worked in close collaboration with the hospital’s professional advisers—architects, structural engineers, services engineers, and quantity surveyors.
In 1965, the Tower Block Building Committee held “two small cocktail parties” to celebrate their 100th planning meeting.21 These small acts of celebration belied the committee’s prevailing mood at the time. The MoH archive is full of lengthy and frustrated back-and-forth messages between the government and Guy’s arguing over the precise design of the building, the timescale of the project, and the available funds. The two sides became increasingly irritated with one another and occasionally the façade of professional detachment slipped. Eventually, the hospital ran out of patience, writing to the ministry:
The Board [of Governors] are very mindful of the country’s current financial difficulties. Nevertheless, they firmly believe that the urgency of the Tower Block scheme is such that it cannot be delayed if Guy’s is to continue to provide the services outlined above. In token of this belief they have, in the present financial stringency, underwritten from their own funds to a total of more than a quarter of a million pounds … so that the building deadline may be met.22
The hospital estimated that the total build would cost £6 million, but they promised the ministry that, due to their financial contributions, the government’s outlay would be less than £4 million: “Finally, by the provision of substantial financial assistance from private funds the Exchequer will be relieved of approximately a quarter of the building cost or more.”23 As the hospital itself put it: “If the Health Service is to derive the maximum value in buildings from the admittedly limited funds available, it would be difficult to find a project providing a better return or better value for money.”24 Worn down by the hospital’s insistence, and persuaded by the influx of cash, the ministry relented and permission was granted for tenders to be invited in 1967. By this point, the building committee had already engaged its architect and the designs had already been drawn. Because they had been willing and able to contribute endowment funds to this large, capital project, Guy’s governors were able to exert considerable influence over the design and pace of the building.


Eventual Structure
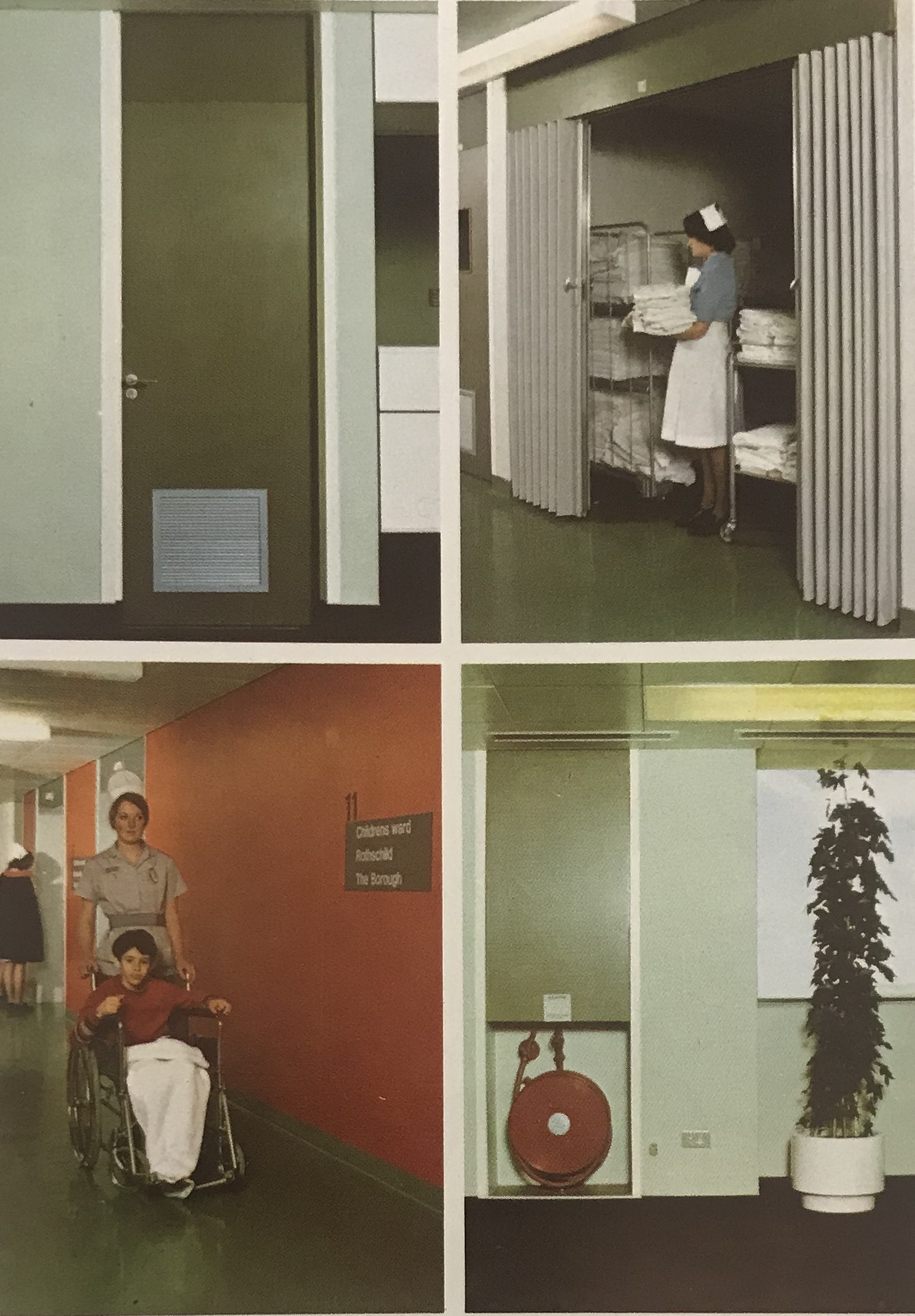
According to the architects, the tower’s design was constrained by the site’s small footprint and evolved from the need to find a building shape that combined a high number of small units of accommodation with a large boiler house requiring a very tall vertical flue. For “practical, as well as aesthetic reasons,” the new building was to be comprised of two linked towers (122 meters and 138 meters tall respectively). The larger, although shorter, tower contained wards, offices, and laboratories in a continuous band around a central core. The shape was designed to “accommodate the requirements of the multi-disciplinary users of the Tower” and included spaces ranging from open-plan offices and teaching areas to single patient rooms. The smaller, although taller, tower was linked at every level to its neighbor, and contained high-speed lifts, reception, and waiting areas. The external finishes of the two towers were designed to be maintenance free. Inside, finishes were also selected to be low effort. Floors were made of PVC tiles, walls painted with fiberglass reinforced paints, and doors were faced with melamine. The use of color was designed to provide a “soft, neutral background in the interior of the Tower.”25 Visual stimulation was provided by furniture fabrics, direction signs, and 1.2-meter square decorative fabric wall-hangings.26 The larger tower had balconies around most floors, intended to reduce glare and solar heat gain and provide access for window-cleaning and firefighting.27
While the hospital was able to expedite the building process, this had unintended consequences. The tower’s structure reflected earlier architectural tendencies. Immediately after the war, bespoke tower-on-podium hospitals predominated, where skyscraper modernity was assumed to “improve patient throughput and clinical efficiency.”28 By the late 1960s, however, this design was slightly outmoded and the MoH attempted to alter Guy’s architectural trajectory, mainly because they thought the twin towers would be too expensive to build and inefficient to run. But they were too late to intervene: decisions had already been made, the hospital had raced ahead with its initial plans, and the money had been spent.
Legacy
Despite the care and attention paid to its design, the finished building was unpopular, both with outside observers, who thought it a brutalist eye-sore, and insiders, who found it an unpleasant place to work. Thirty years later, in 2008, the building’s façade was showing significant signs of decay. Guy’s embarked on a £40 million capital investment project to reclad the building’s concrete exterior. Architects Penoyre & Prasad, working with engineering firm Arup, reskinned the building, repairing sizeable cracks that had formed in the walls.
Sunand Prasad referred to the tower as an “ugly building designed with a great deal of love.” This is an accurate epithet. Guy’s Tower became a symbol of the postwar NHS on the London skyline, embodying both a commitment to clinical efficiency and modernity as well as the intransigence of the British state. The NHS was intended to be a rational, top-down system—and is often imagined as such—but it is also a patchwork of local legacy institutions that persist in spite of their partial historical effacement. Indeed, just as Guy’s Tower mirrors the postwar NHS, the postwar NHS reflects Britain as a whole.
But, perhaps more importantly, Guy’s Tower also represents the uneasy place of “love” in the ideologies and practices of the NHS. On the one hand, the influence of utilitarianism on the foundations of the NHS replaced the vague notion of “love” or commitment with a normative concept of benefit and a calculus for its ideal distribution. On the other, an alternative, more capacious, and more directly emotional idea of love still permeates the NHS, which shapes the interpersonal relationships between healthcare professionals and patients and is instrumentalized by politicians of all persuasions. More simply, hospitals are places where the benevolence of the welfare state is supposed to most directly benefit citizens, but this specific hospital building also demonstrates the largely unrecognized truth that the NHS was, and remains, underpinned by charity.
Agnes Arnold-Forster and Caitjan Gainty, “To Save the NHS We Need to Stop Loving It,” Renewal: A Journal of Social Democracy 29, no. 4 (2021): 53–61.
Rowena Mason, “Boris Johnson leaves hospital as he continues recovery from coronavirus,” The Guardian, April 12, 2020.
David H. Solkin, “Samaritan or Scrooge? The Contested Image of Thomas Guy in Eighteenth-Century England,” The Art Bulletin 78, no. 3 (1996): 467–84.
John Mohan, “Geography and Social Policy: Spatial divisions of welfare,” Progress in Human Geography 27, no. 3 (2003): 363-374.
Alistair Fair, “‘Modernization of Our Hospital System’: The National Health Service, the Hospital Plan, and the ‘Harness’ Programme, 1962–77,” Twentieth Century British History 29, no. 4 (2018): 547–75.
Charles Webster, The Health Services Since the War, Volume 1: Problems of Health Care: The National Health Service Before 1957 (London: HMSO, 1988).
Quoted in Fair, “‘Modernization of Our Hospital System’,” 547.
Jonathan Hughes, “The ‘Matchbox on a Muffin’: The Design of Hospitals in the Early NHS,” Medical History 44, no. 1 (2000): 21–56.
Fair, “‘Modernization of Our Hospital System’.”
Fair, “‘Modernization of Our Hospital System’.”
National Health Service, A Hospital Plan for England and Wales, Command 1604 (London: HMSO, 1962).
Quoted in Fair, “‘Modernization of Our Hospital System’.”
National Health Service, A Hospital Plan for England and Wales.
Fair, “‘Modernization of Our Hospital System’.”
Fair, “‘Modernization of Our Hospital System’;” Ed DeVane, “Pilgrim’s Progress: The Landscape of the NHS Hospital, 1948–70,” Twentieth Century British History 32, no.4 (2021): 534–552.
Fair, “‘Modernization of Our Hospital System’.”
David Edgerton has critiqued the declinism of Britain’s twentieth-century historiography. David Edgerton, The Rise and Fall of the British Nation: A Twentieth-Century History (London: Allen Lane, 2018).
Department of Health for Scotland, Hospital Endowments: Report of the Hospital Endowments Commission (Edinburgh: HMSO, 1955), paragraph 26. See also Bernard Harris and Rosemary Cresswell, “The legacy of voluntarism: Charitable funding in the early NHS,” Economic History Review 77 (2024): 554–583, 574.
TNA MH99/37, “NHS: Appeals for funds, etc.,” para. 2 (18/12/48) (RHB (48) 41A; HMC (48) 25A; BG (48) 23A).
Endowments Committee Minutes, May 1963–March 1968, H09/GY/A/342/005, London Metropolitan Archive.
Endowments Committee Minutes, May 1963–March 1968, H09/GY/A/342/005, London Metropolitan Archive.
Ibid.
Ibid.
Ibid.
See Victoria Bates, “Cold White of Day: White, Colour, and Materiality in the Twentieth-Century British Hospital,” Twentieth-Century British History 34, no. 1 (2023): 1–37.
Bates, “Cold White of Day.”
“Guy’s Tower,” 1976, H09/GY/A/365/025, London Metropolitan Archive.
Hughes, “The ‘Matchbox on a Muffin’.”
Treatment is a collaboration between e-flux Architecture, the Institute for the History and Theory of Architecture (gta), ETH Zürich (2021 and 2025), and Istituto Svizzero, Rome (2025).