What would it mean to design buildings that exceed the economic accountings of liberal biopolitics, that instead offer an entirely different rationale for supporting health? In the years that Michel Foucault conceptualized the term biopolitics, he was part of a constellation of researchers and architects who developed care praxes that defined the value of life and its maintenance through a desire-based calculus. The welfare state institutions of architect Nicole Sonolet in particular—mental hospitals, public housing complexes, and new village typologies built mainly in postwar France and postcolonial Algeria from the 1950s to the 1980s—were designed not only to support, but to center the needs of people often excluded from design processes.1 Sonolet’s mental health centers for residents of Paris’s 13th arrondissement in particular were key projects for discovering a design practice tied to the provision of care for its own sake.
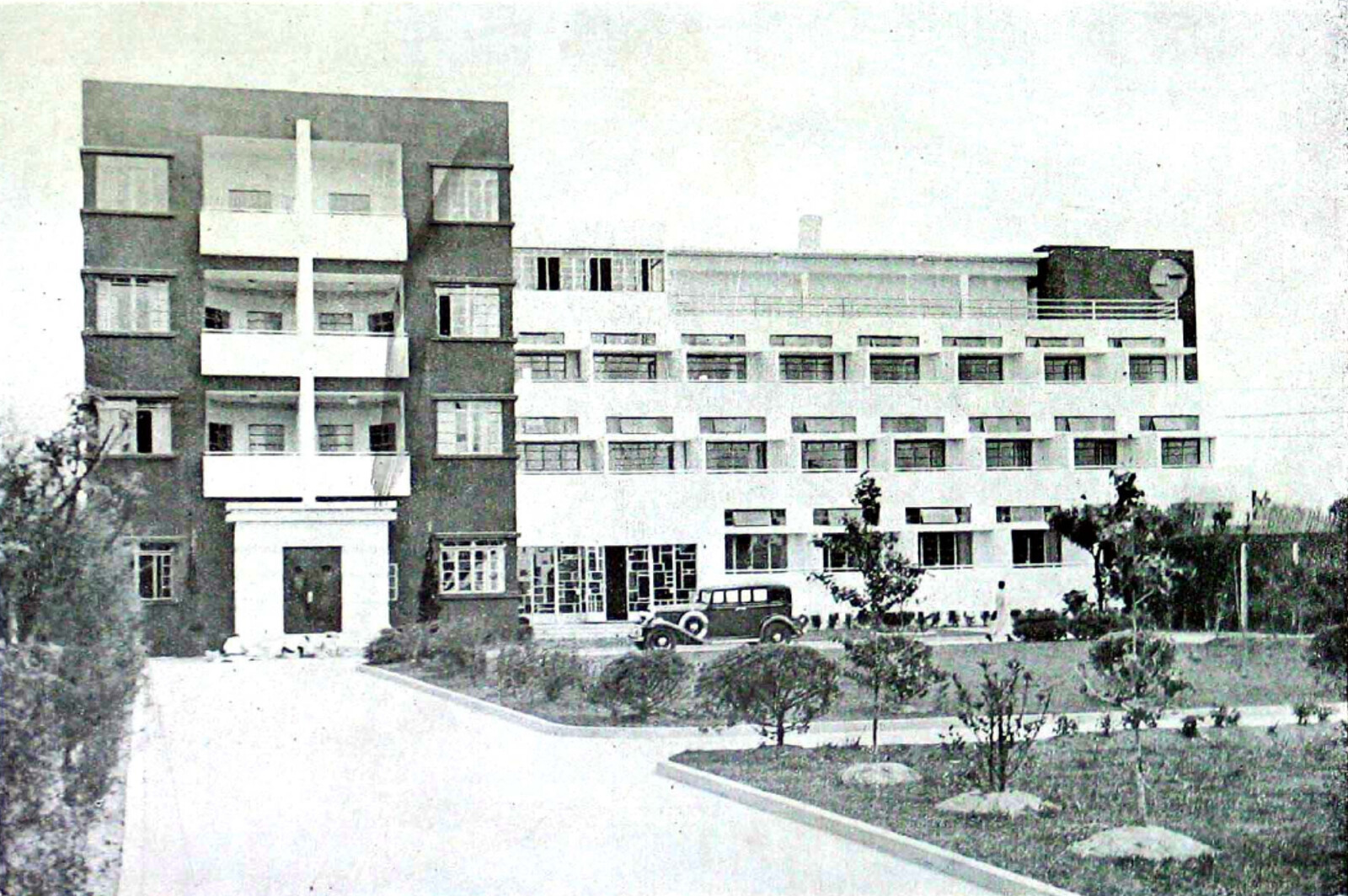
Although her work is formally sophisticated and theoretically rich, Sonolet’s work is not well known. She was admitted to study architecture at Ecole de Beaux Arts in Paris in 1944, but her studies were interrupted by the Second World War; she completed her thesis project for a psychiatric hospital in 1954. During the postwar years and into the 1960s, she designed mid-sized subsidized housing complexes in the Parisian suburbs as well as private houses, which helped to fund her practice. In those years she also returned to the subject of her thesis, and began to design mental health care facilities. Her first major mental hospital was l’Eau Vive, located in the Parisian suburb of Soisy-sur-Seine, which she began to work on in conversation with the psychiatrist Phillippe Paumelle starting in 1958. In the late 1960s and early 1970s, she and Paumelle collaborated again to build the Center for Mental Health of the Association de Santé Mentale 13 (or ASM 13) in Paris, a compliment to l’Eau Vive which was focused on outpatient care. In these years, Sonolet also published articles on social housing and the architecture of mental health, conducted research on environmental psychology, and taught at the Ecole Speciale d’Architecture and the Ecole de Beaux-Arts, serving meals to striking students during 1968 from her kitchen.
Sonolet’s interest in mental healthcare was intellectual as well as personal (a close relative had been hospitalized), and she was dedicated to advocating for more humane treatment for depressive, psychotic, and schizophrenic patients. In the course of her thesis research, she met with leading thinkers in the institutional psychotherapy (IP) movement, including Paumelle. IP practitioners sought to treat patients within their social and political contexts, and to use all of the interactions around psychotherapeutic care (including the space of the hospital or clinic, the exchanges a patient might have with a physical therapist, a house keeper, or an art teacher) as a means of rebuilding damaged social and relational bonds, empowering patients to develop their own courses of healing in collaboration with their doctors.2
Following IP innovators Francois Tosquelles and Frantz Fanon, Paumelle was particularly dedicated to offering community-based care. He saw it as a key alternative to the isolation and neglect patients too often endured in French asylums. The rural location of asylums forced patients to leave their communities and families, and they often received inconsistent treatment from rotating teams of doctors and nurses. As part of an international movement advocating for community-based care, Paumelle hoped to provide patients with consistent medical teams, outpatient psychotherapy, and free clinics, as well as occupational therapies as a means of limiting hospitalization. He made this argument using the rationale of the national budget: this would save costs, since local outpatient care was far less expensive than hospitalization, while at the same time increasing the availability of services. The French state did shift to support a policy of distributing care facilities regularly throughout geographic “sectors” later in the 1960s, but Paumelle was only able to begin setting up the system he imagined with private support. In 1958, with assistance from a donor who wanted to improve treatments for alcoholics, he founded the Association de Santé Mentale 13, a non-profit organization intended to serve the mental healthcare needs of the population of the 13th arrondissement in Paris. This enabled Sonolet and Paumelle to begin to plan l’Eau Vive, which would be the ASM 13’s first hospital, and would serve as a kind of testing ground for community care typologies.


Paumelle had hoped to be able to situate the ASM 13’s hospital in Paris, close to the population it would serve. But when land made was made available in the verdant park-like landscape of a former theological center in Soisy-sur-Seine, a suburban town just south of Paris, they accepted the opportunity to create a hospital outside the city. For l’Eau Vive, Sonolet designed a campus with ten new buildings intended to serve 175 patients. A series of low, rectilinear pavilions housed a welcome center, housing for doctors and staff, a social center and cafeteria (which would allow doctors a chance to casually exchange ideas), an administration building, and five separate residential treatment buildings, each overseen by a different team of doctors and nurses.3 Within these residential treatment buildings, patients were organized into groups of seven and monitored by one consistent nurse rather than a rotating team of staff, as Paumelle and Sonolet believed that deeper and more therapeutic relationships could form with consistent care teams. In order to design the complex, Sonolet interviewed doctors, nurses, and staff working in the hospital to understand the particular burdens of caregiving. She intended for the design to offer them opportunities to recharge from care and to escape from patients when necessary, which would counterbalance the fact that they would make themselves available to patients outside of structured treatment times.
This clinic would not be a “closed” one, in the carceral manner of old asylums, where patients were primarily confined to their rooms, but rather would encourage movement both within the buildings and on the grounds, a kind of healing circulation that echoes that of post-miasma theory hospital design. This decision was not made out of a fetishization of movement, but rather because Sonolet and Paumelle believed that patients had the right to evolve emotionally in the course of their treatment. If they were not fixed in one space in the hospital, supposedly, they also would need not remain in one fixed mental state or diagnosis. This idea of movement drove the design of the hospital. Sonolet theorized that architectural and interior design could “condition” spaces and provide a variety of experiences: of openness to the world or of enclosure; of stimulation or of repose; of warmth or of coolness. In the course of her design research, doctors would explain to Sonolet the kinds of phenomenological qualities they hoped to offer. She would then develop designs for these spaces, and then once built, patients would move through the hospital to spend time in places with the qualities they desired. Different materials, configurations of light, visual privacy, noise levels, and activities would all contribute to patients’ emerging understanding of how they could use space in the course of their own treatment. Moving from a more isolated state to a more socially-engaged space would, in theory, help prepare patients to reintegrate in their communities.
All of these “conditions” could be rendered in a largely modernist architectural vocabulary. In break rooms, for example, chairs could be grouped and regrouped to offer flexible possibilities for socialization; bedrooms would be set up so that patients could keep the door open to be “open” to others while still maintaining some visual and aural privacy; windows could be opened or closed to allow for connection to the landscape; common bathrooms would allow both for larger, sunnier bedrooms and bring the patients into contact with others. Even though Soisy was far from Paris, Paumelle and Sonolet hoped that on its insides and between its pavilions, it could still model the forms of community immersion that would be possible in an urban mental health center. Even though bucolic, it was urban, and urbanity was healing.
After the initial phase of construction was complete in 1963, Sonolet began to publish conclusions from her experience constructing Soisy and her conversations with IP practitioners in journals of architecture and psychology.4 She became known as an expert in the architecture of these new practices of mental health, and frequently consulted with international researchers interested in the intersections of architecture and mental healthcare. Her expertise was well-known to Félix Guattari, who a few years after the opening of l’Eau Vive founded a group called CERFI, or the Centre d’études, de recherches et de formation institutionnelles (Center for Institutional Studies, Research, and Training). Guattari had worked closely with many of the key protagonists of IP at the clinic of La Borde starting in the mid-1950s. His analytic beliefs were slightly more radical than Paumelle’s, but he considered Sonolet a friend and admired colleague, exchanging letters with her about various CERFI projects, and drawing on her knowledge to organize an early issue of the group’s journal, Recherches, on architecture, programming, and psychiatry.5


Programming Collective Facilities
The 1967 issue of Recherches was one of CERFI’s first deep investigations of “programming,” a special term for the group that encompassed architectural as well as other forms of planning.6 As part of a discussion about how mental health infrastructure should be incorporated into the city, the issue put Sonolet in dialogue with psychiatrists and practitioners of institutional psychotherapy, as well as the architects Aymeric Zublena, Alain Schmied, Alain Fabre, and Albert Schwartz. Sonolet’s contribution to the journal reprised material she had previously published based on her work at l’Eau Vive, outlining challenges, processes, and formal considerations that would be necessary when programming hospitals, along with a menu of programmatic possibilities and several charts schematizing how such a scheme could work with different population densities.7 She stressed that long-term success could only be achieved after considerable research and conversation. While she was knowledgeable about mental health design, geographies and care strategies varied across France, she was clear that no architect could offer a fixed program or typology that could be derived without deep conversation with doctors and staff. From this publication, Sonolet’s insights about programming became part of a much larger conversation within the CERFI.
While CERFI was started by Guattari, it was led by a large, interdisciplinary group of militants, activists, sociologists, historians, writers, and psychoanalysts. They shared a desire to reform the instruments of the French state via new combinations of institutional, historical, sociological, and psycho-analysis, as well as through philosophy, critique, conversation, and design. The group received significant funding from the French government to develop projects and research—somewhat surprising given that they interrogated the state’s various projects of normalization and alienation. Nonetheless, a funder at the Ministère de l’Équipement (Ministry of Public Works) was intrigued by CERFI’s work on équipements collectifs (collective facilities, or infrastructures).8 The Ministry hoped to build evidence for developing this infrastructure and to understand its forms, lifecycles, and potential impact on everyday life. CERFI hoped to use this funding to rethink the relationship between infrastructure and power through emerging critical discourses, rethinking Althusserian and Lacanian theories of subject formation in the context of praxis.
CERFI’s first research contract from the Ministry of Public Works in 1971, Programmation des équipements collectifs dans les villes nouvelles – les équipements d’hygiène mentale (Programming collective facilities in New Towns – facilities for mental health), offered a significant opportunity to develop architectural ideas about spaces for mental health.9 The goal of this project was to discuss how to plan community mental health facilities not just as pilot projects, as Sonolet and Paumelle had done at l’Eau Vive, but on a national scale. Sonolet supported this project, and shared insights from her research on mental health architecture, especially about the necessity for private spaces, access to greenery and light, and the scale of patient-doctor units. However, she and another architect-interlocutor, Alain Schmied, both argued against the idea of mental health typologies: there was no architectural formula that could translate health into space. Rather, Sonolet explained, spaces had to be developed through a conversational programming process, one that would elicit the desires of both clinicians and patients, and whose outcome was not known in advance. In other words, the design of mental health architecture had to be akin to the open-ended practices of institutional psychotherapy itself. Discussion about programming mental health facilities offered CERFIstes opportunities to transfer architectural ideas into institution-building techniques adapted from institutional psychotherapy, and vice versa.
CERFI’s subsequent work on other kinds of collective infrastructures drew from this early work on community mental health. From 1971–1976, they organized an integrated child care center in the New Town of Melun-Sénart, which combined day care facilities, leisure facilities for children, a school, child protection services, and after-school care; they studied Alma-Gare, a neighborhood of worker housing in Roubaix, and proposed programmatic and architectural strategies for improvement; they planned mental health facilities in new towns (work which led partially to the development of similar services in Paris); and they helped preserve a workers’ retreat and establish a cultural center at the Buisson Farm outside the former Menier Chocolate Factory in Noisiel. In all of these projects, CERFIstes sought to understand how shared infrastructures might structure different practices of liberation, remaking the family, the neighborhood, and the clinic. All of this work was interdisciplinary, with architects participating on research teams alongside historians, philosophers, doctors, artists, urbanists, and many others.
Some of CERFI’s funding was also funneled to Michel Foucault. His 1973–1974 research seminar “Recherche sur l’institution hospitalière à la fin du XVIIIe siècle, généalogie des équipements collectifs” (“Research on the Institution of the Hospital at the End of the Eighteenth Century: Genealogy of Public Amenities”), was partially funded by the group, and it was in the course of this seminar—and conversations with architects and architectural historians (though not Sonolet)—that he developed the term biopolitics. Seminar participants—Blandine Barret-Kriegel, the architects Bruno Fortier and François Béguin, and Foucault’s niece Anne Thalamy—analyzed architectural plans, medical proclamations, and state records in order to elaborate a history of the belief that architecture was one of several dispositifs or apparatuses capable of producing health-effects in the body of the population. The results of this research were published as a book, Les machines à guérir: aux origines de l’hôpital moderne (Curing Machines: On the Origins of the Modern Hospital) in 1976.10 Foucault’s essay, “The Politics of Health in the Eighteenth Century,” introduced the research and argued that biopolitics particular to the late eighteenth century were elaborated through the medicalization of space and the subsequent creation of spatial-medical dispositifs, or material and institutional instruments. Once life was capable of being prolonged through the eighteenth-century hospital, he claimed, life itself it could be conceived of as a controllable value capable of being modulated across a population.
Bruno Fortier, a co-organizer of the seminar, developed conclusions related to the discipline of architecture out of the group’s research. In his chapter “The Architecture of the Hospital,” he described the process by which the design of hospitals was standardized, showing how control over hospital design shifted from being the purview of architectural professionals to becoming a medical concern, and then, once deemed important enough, again the purview of architects.11 Fortier made an implicit connection between understandings of the social effects of architecture in the eighteenth century and understandings of these effects in twentieth-century modern architecture, arguing that architectural standardization produced the idea of a perfectible architectural type.12 An eighteenth-century idea of a perfectible type, Fortier argued, allowed for a conceptualization of program and organization as something separate from previously “architectural” concepts of order or decoration. Thus, the political importance of the hospital’s health-effects did not just extend to the bodies of citizens, as Foucault had elucidated in his essay, but also helped eighteenth-century architects make a claim that there was an ideal form for a particular program, the very idea which Sonolet and Schmied had countered in CERFI’s 1971 research project on mental health in new towns. Foucault and Fortier explained that there had been an eighteenth-century fantasy of a spatial “curing machine,” which created a belief that there was a cause-and-effect relationship between health outcomes and architectural design. But their analyses make clear that rather than a reality, this was an idealized discourse about the design of the operation of government; architecture was not a machine, and architecture alone could not produce forms of behavior or new political realities. Fortier left out the colonial dimensions of this fantasy of machinic control—ones essential for extracting value from land and life, and particularly Black lives, from a distance.13
I do not know if Fortier was in dialogue with Sonolet and Schmied, or how aware he was of CERFI’s 1971 research, but his analyses did compliment and intensify their conclusions about programming. Fortier’s genealogy shows that the idea of programming had a long history of being reclaimed by practitioners of various disciplinary backgrounds, and that architecture in France had long been open to concerns that seemed to be outside of its disciplinary purview. CERFI’s research project on mental hospitals in new towns anticipated and contributed to Foucault’s first theorization of the term biopolitics. While Guattari, Schmied, Sonolet, and the doctors they collaborated with did not coin this term, from the beginnings of their conversations it is clear that Sonolet and the CERFIstes were trying to produce alternatives to a neoliberal biopolitical calculus where decisions about governance were made according to monetary value assigned to life. This valuing of life justified the French state’s construction of infrastructure like the eighteenth-century hospitals Foucault and Fortier described, as well as the twentieth-century research contracts that CERFI received to install mental health services in new towns. In contrast, Sonolet’s hospitals and CERFI’s équipements collectifs were organized around the provision of care for its own sake, demonstrating that another rationale for care was possible.


The Center for Mental Health
CERFI did not ultimately manage to create nationwide programs for mental health services. Their funding decreased precipitously alongside French state funds for mental healthcare in the early 1970s. However, around this time, private philanthropy allowed Sonolet and Paumelle to build the urban mental health complex for the ASM 13 that they had also hoped to construct in the late 1950s: the Center for Mental Health, located on Avenue Edison near the Place d’Italie.14 Sonolet had long worked on conceptual plans for an urban counterpart for l’Eau Vive, but now, with a site and a sponsor secured, she and a design collaborator, Maria Baran, drew up detailed plans for which they received construction permits in 1972. This complex both inspired and bears traces of CERFI’s work on collective facilities. The Center for Mental Health offered outpatient and emergency residential services for residents of the 13th arrondissement, allowing patients the ability to remain in their communities while receiving care. The complex combined two treatment centers, one for adults and the other for children (named respectively for Albert Binet and Phillippe Paumelle, after his premature death in 1974), as well as a psychoanalytic institute and family support clinic. Even though the Center for Mental Health was supposed to make up for the lack of urbanity at l’Eau Vive, it also attempted to import a trace of its pastoral aesthetics into an urban setting: as part of the project, a new public park was built on an adjoining parcel of land in 1973. The park made the project more palatable to neighborhood residents, who received a much-needed green space, but it also made it possible for Sonolet and Baran to open the building to light and air. Doctors, patients and staff could look out onto planted spaces during treatment, as they had at l’Eau Vive.
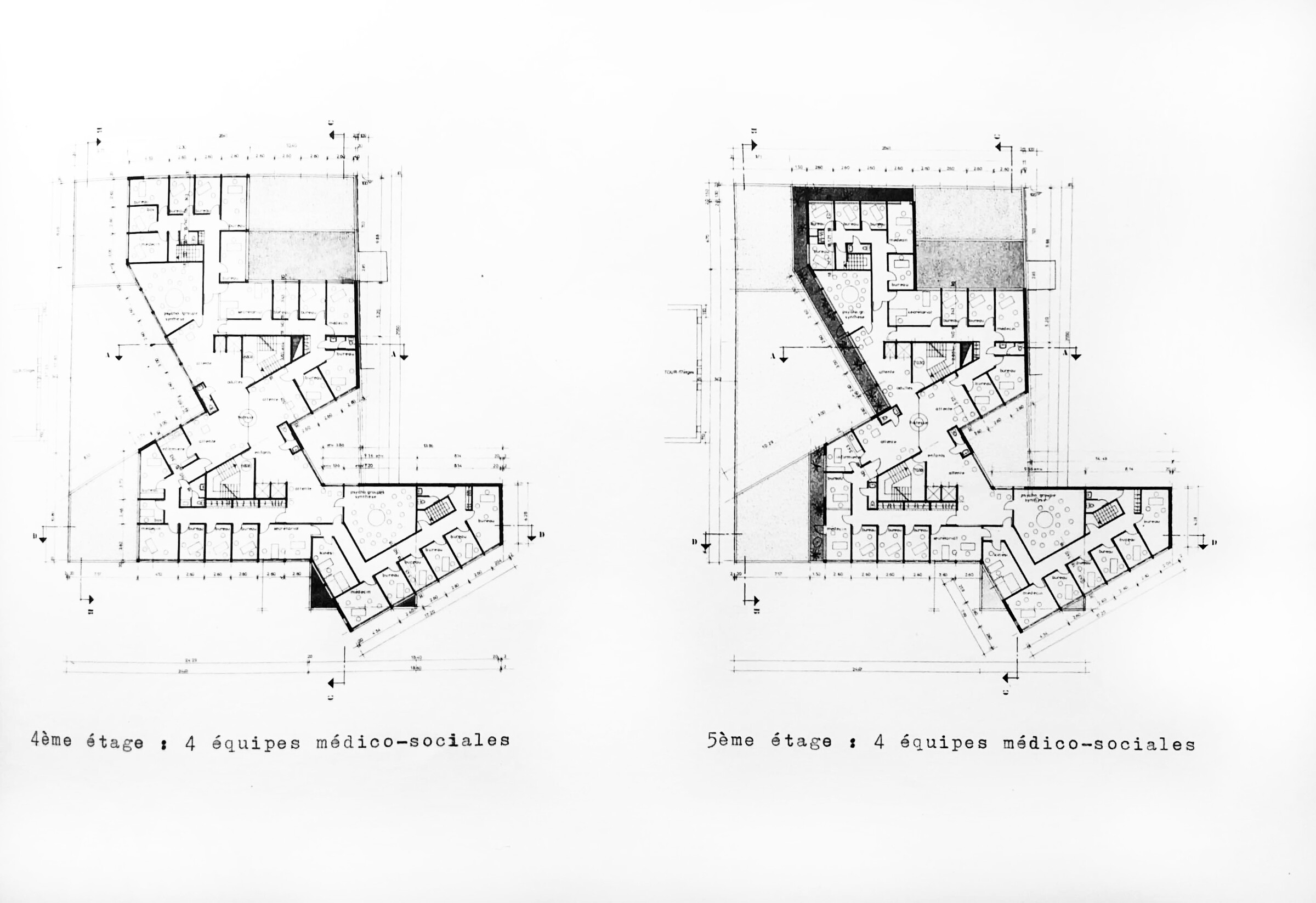
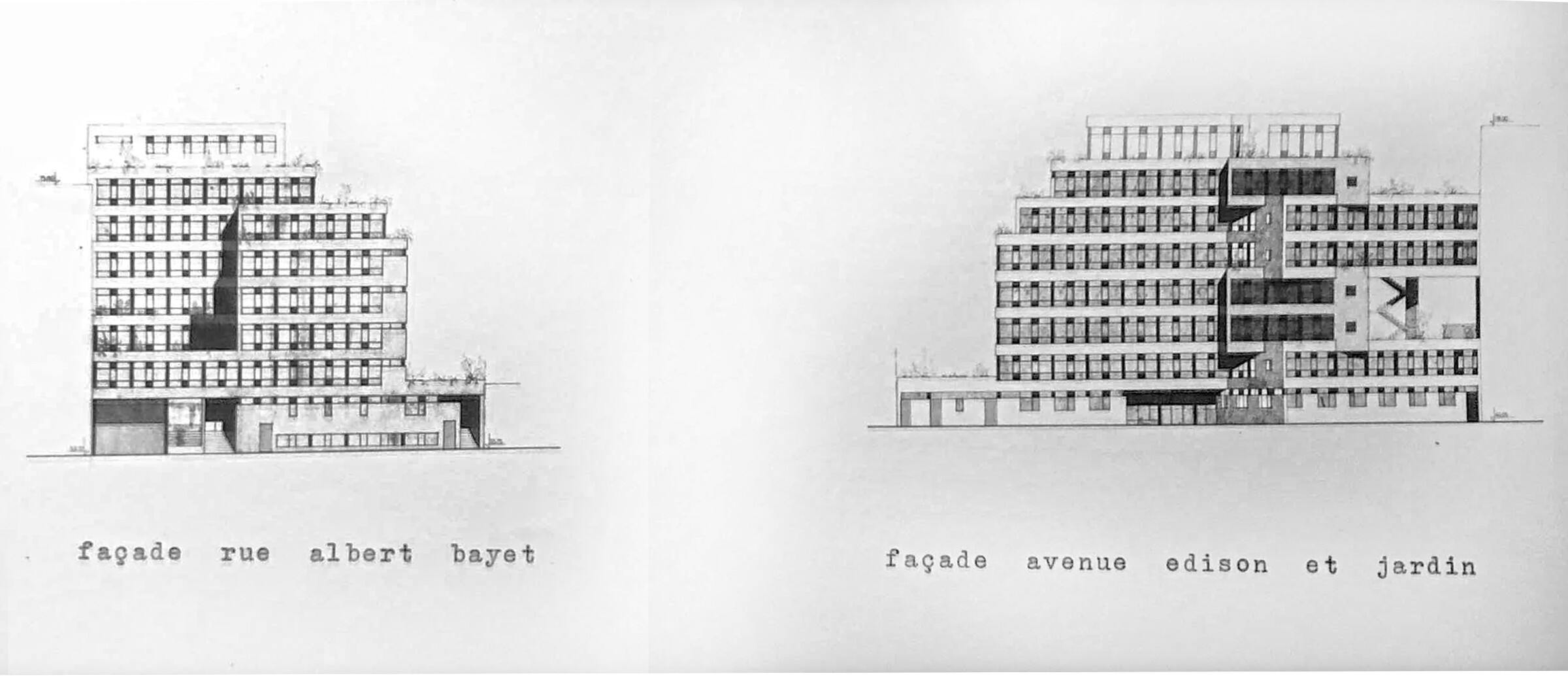
The geometry of the Center for Mental Health is much more complex than that of the rectilinear pavilions of l’Eau Vive. Treatment spaces and offices rotate around two central stair cores, and the building steps back as it rises, allowing light to fall on terraces and outdoor planted spaces that line the building and buffer the offices, waiting rooms, and treatment areas from the street. Triangular forms jut towards the street to create a variegated and lively façade, one that perhaps signified the particularity and unpredictability of treatment paths espoused by practitioners at ASM 13. On the interior, waiting rooms fill the negative space of the exterior angles, offering patients semi-private corners with views to terraces or the public gardens in which to wait. The complex also featured spaces for teaching, including an auditorium, library, classrooms and meeting rooms, as well as several spaces for group psychotherapy on each floor. The top floor featured a restaurant and cafeteria for staff, facilitating interaction between the many doctors that would use the space but who might not speak to each other as readily if they left the complex to eat.
Much of the treatment at the Center for Mental Health was done in private offices, which in spite of the angular facades were mostly rectilinear and set along the street-facing sides of the buildings. Patients would have been able to enjoy the vegetal views onto planted terraces from a therapy session, and perhaps also in some cases, walk from an office onto a terrace. As she had at l’Eau Vive, Sonolet tried to ensure staff needs were met in her design. The terraces were planned to offer doctors and staff visual repose for times when the psychic interiors they inhabited became too overpowering. The presence of planted terraces at street level not only buffers the hospital, but also suggests that spaces for mental health can offer amenities even to residents that didn’t directly partake in them. Sonolet’s and Baran’s gardens helped to ease and to normalize the provision of care.


Exterior of the Center for Mental Health, Paris. Photograph by author.
Because of its condensed footprint, and because treatment was largely done in a single room, as well as over a short duration, the Center for Mental Health didn’t offer patients the healing circulation that was a key part of residential treatment at l’Eau Vive. This was in part because the patients who used the Center for Mental Health were less sick, and could manage with only outpatient treatment; spending less time in the building would mean that it would not need to offer as many treatment resources. The clinic therefore did not present itself as a dispositif for healing, a space that would be activated through creative use and misuse. A patient could not write her own treatment path through the building. If she wanted to do so, she would need to leave the clinic, to experience the city itself, to use it as a form of treatment. Equipements did not just support the city; they were the city.
Sonolet, Foucault, and the CERFIstes connected architecture and infrastructure to health and subjectivity. While we are more familiar with stories of how late twentieth-century architects borrowed so-called “French Theory,” looking at its history reveals just how much architectural thought and practice contributed to its theories of power, and how much a preoccupation with illness fueled these inquiries. Nicole Sonolet’s spaces of care, along with CERFI’s work on équipements collectifs helped generate a theory of infrastructure that was not biopolitical, but instead based on both care and desire. This beyond-biopolitical practice likely shaped Foucault and Fortier’s historic work about hospitals, sharpening their work into not just theory, but critique of emerging neoliberalism in France. In turn, knowledge of CERFI’s beyond-biopolitical practice may have informed Foucault’s theories of biopolitics. Research on collective facilities, completed with architectural methods, spurred important ideas that circulate today in many other fields.
These feedback loops between critique, analysis, programming, and design had parallels with the patient-specific treatment protocols that IP practitioners developed as they worked against the idea of a uniform and standardized formula for treating different illnesses. Sonolet seemed to modify the psychoanalytic practice of providing care to derive a process for designing hospitals. Following the principles of IP, this would yield designs that were guided by a set of common principles, but specific to each situation and team of staff members, as well as the community from which they issued. Designing these spaces required close collaborations. This helps to account for the formal variations in Sonolet’s work, and the careful intentionality of her designs. Ideally, implied Sonolet, the processes of design care that generated formal variety might be deployed in the planning of all collective facilities.
This article condenses arguments and analysis from several lectures given from 2018- 2020, as well as previously-published texts: Meredith TenHoor, “State-Funded Militant Infrastructure? CERFI’s Équipements Collectifs in the Intellectual History of Architecture,” The Journal of Architecture 24, no. 7 (October 3, 2019): 999–1019; Meredith TenHoor, “Des architectures du soin: Philippe Paumelle et Nicole Sonolet,” Terrain 76 (Spring 2022); Meredith TenHoor, “Architecture and Biopolitics at Les Halles,” French Politics, Culture & Society 25, no. 2 (2007): 73–92. I am grateful to the editors of these publications for permission to summarize them here, and to Christine de Bremond d’Ars, for sharing her insights and Sonolet’s archives with me.
For more on the theories and politics of IP, see Valentin Schaepelynck, L’institution renversée: Folie, analyse institutionnelle et champ social (Paris: Eterotopia, 2018), and Camille Robcis, Disalienation: Politics, Philosophy, and Radical Psychiatry in Postwar France (University of Chicago Press, 2021).
For more detail on the design of L’Eau Vive, see Meredith TenHoor, “The Design of Community Mental Health Care: Nicole Sonolet in Postwar France,” gta papers 7 (Zurich: gta Verlag 2022), and Julie Mareuil, “Une clinique-pilote de la sectorisation psychiatrique: L’hôpital de l’Eau Vive et son évolution de 1959 à 1977” (MA Thesis, ENSA Paris-La Villette, 2020).
Nicole Sonolet, “Un centre de santé mentale. Point de vue et proposition d’un architecte,” Information Psychiatrique 6 (June 1966): 527–532; Nicole Sonolet, “An Urban Mental Health Center: Proposal for an Experimental Design,” Social Psychiatry 2, no. 3 (1967): 137–143.
CERFI, “Programmation, Architecture et Psychiatrie,” Recherches 6 (1967).
Susana Caló and Godofredo Pereira offer a helpful analysis of this issue of Recherches, focusing on how CERFI modified ideas about mental health and its place in urban design and planning in France. See Susana Caló and Godofredo Pereira, “CERFI: From the Hospital to the City,” London Journal of Critical Theory 1, no. 2 (May 2017): 83–100.
Nicole Sonolet, “Un centre de santé mentale urbain: proposition d’une experience,” Recherches 6 (1967).
CERFI’s work on this topic caught the attention of the landscape historian Michel Conan, who was in charge of urban research at the Ministry of Public Works. Conan arranged funding for CERFI to undertake projects to plan mental health facilities in the New Towns of Évry and Melun-Sénart. For more detail, see TenHoor, “State-Funded Militant Infrastructure?”
CERFI had to submit official reports of the work completed for their various research contracts, and did so in this case by publishing a small booklet: CERFI, “La programmation des équipements collectifs dans les villes nouvelles (Les équipements d’hygiène mentale): Rapport sur l’exécution de la convention d’études entre le CERFI et le Ministère d’équipement et du logement (Direction de l’aménagement foncier et de l’urbanisme) du 4 mai 1971” (Paris: Centre d’études, de recherches et de formation institutionnelles, 1972).
Michel Foucault, ed., Les Machines à guérir: aux origines de l’hôpital moderne, (Paris: Institut de l’environnement, 1976). Foucault’s essay has been translated in English as Michel Foucault, “The Politics of Health in the Eighteenth Century.” In: Power/Knowledge : Selected Interviews and Other Writings, 1972-1977, trans. Colin Gordon (New York: Pantheon Books, 1980). A translation of the entire text, edited and introduced by Anne Kockelkorn and Moritz Gleich, is forthcoming, and eagerly anticipated.
Bruno Fortier, “Architecture de l’hôpital.” In: Les machines à guérir : aux origines de l’hôpital moderne (Paris: L’institut de l’environnement, 1976).
Ibid., 72.
This is equally true of Foucault’s theories of biopolitics which miss many of the most crucial sites of eighteenth century biopolitical formation, particularly those of extractive economies and enslavement, as Alexander Wehilye, Simone Brown, and many others have documented. See Simone Browne, Dark Matters: On the Surveillance of Blackness (Durham: Duke University Press, 2015); Alexander G. Weheliye, Habeas Viscus Racializing Assemblages, Biopolitics, and Black Feminist Theories of the Human (Durham: Duke University Press, 2014). However, CERFI’s and Sonolet’s resistance to theories of machinic governance aligned with their anti-colonial stances more generally.
Sonolet collaborated with architect Maria Baran on the project; later they were joined by Olek Kujawski and Tristan Darros who oversaw construction. Permits for the project were approved in 1972, but because of funding and other challenges, it took nearly nine years for the project to be completed.
Sick Architecture is a collaboration between Beatriz Colomina, e-flux Architecture, CIVA Brussels, and the Princeton University Ph.D. Program in the History and Theory of Architecture, with the support of the Rapid Response David A. Gardner ’69 Magic Grant from the Humanities Council and the Program in Media and Modernity at Princeton University.